
Which Therapy Is Best for Anxiety? A Complete Guide
Which Therapy Is Actually Best for Anxiety? Let’s Cut Through the Noise
If you have typed “which therapy is best for anxiety” into a search engine recently, you already know the problem. The results are a wall of conflicting information — listicles recommending everything from CBT to crystal healing, therapy directories optimized for clicks rather than clinical accuracy, and enough acronyms (CBT, DBT, ACT, EMDR, IFS, ERP, MBCT) to make your head spin before you’ve even started.
Meanwhile, you are anxious. Possibly exhausted from being anxious. Possibly anxious about being anxious. And the last thing you need is another overwhelming research project standing between you and actually getting help.
This article exists to cut through all of that honestly and directly.
The answer to “which therapy is best for anxiety” is not one-size-fits-all — but it is also not infinitely complicated. The research is actually quite clear on what works, for which presentations, and why. What most people are missing is not access to that research — it is a clear, honest translation of it into something they can actually use to make a decision about their own care.
That is what this article provides.
What Is Anxiety, Really? Understanding the Target Before Choosing the Treatment
Before comparing therapies, it is worth establishing what anxiety actually is — because the most common misunderstanding about anxiety (that it is simply excessive worry or nervousness) produces mismatched treatments and disappointing outcomes.
Anxiety is a neurobiological condition rooted in the dysregulation of the brain’s threat-detection and stress-response systems. At its center is the amygdala — the brain’s alarm system — which in anxiety disorders fires too easily, too intensely, and too persistently in response to stimuli that the rational brain recognizes as non-threatening.
The result is a system perpetually calibrated for danger that isn’t there. Heart racing during a work presentation. Stomach turning before a social gathering. Lying awake at 3 a.m. catastrophizing about things that haven’t happened. Avoiding situations that the anxious brain has tagged as threatening — and finding that the world slowly shrinks as avoidance expands.
Two mechanisms sit at the heart of almost every anxiety disorder:
Cognitive distortion: The anxious brain consistently overestimates threat and underestimates capacity to cope. It generates worst-case interpretations automatically, before conscious reasoning has a chance to intervene.
Behavioral avoidance: The anxious person avoids the situations, sensations, and thoughts that trigger anxiety — which provides short-term relief and long-term maintenance of the anxiety, because avoidance prevents the brain from learning that the feared situation is actually safe.
Every effective therapy for anxiety targets one or both of these mechanisms. Understanding this makes it much easier to evaluate what you’re being offered and why.
The Anxiety Disorders: Not All Anxiety Is the Same
Anxiety is not a single condition. The DSM-5 identifies several distinct anxiety disorders, each with specific features that influence treatment selection:
Generalized Anxiety Disorder (GAD): Chronic, pervasive worry across multiple life domains — health, finances, relationships, work — that is difficult to control and accompanied by physical symptoms including muscle tension, fatigue, and sleep disruption.
Panic Disorder: Recurrent, unexpected panic attacks — sudden surges of intense fear with dramatic physical symptoms — combined with persistent fear of future attacks and avoidance of situations associated with attacks.
Social Anxiety Disorder: Intense fear of social or performance situations in which the person might be scrutinized or judged negatively by others, leading to significant avoidance of social interaction.
Specific Phobias: Marked fear of specific objects or situations — heights, flying, needles, animals — that is disproportionate to the actual threat and produces avoidance.
Agoraphobia: Fear and avoidance of situations where escape might be difficult or help unavailable during a panic attack — crowds, public transport, open spaces, being outside the home alone.
Health Anxiety (Illness Anxiety Disorder): Excessive preoccupation with having or developing a serious medical illness, accompanied by health-checking behaviors, reassurance-seeking, and significant distress.
OCD (Obsessive-Compulsive Disorder): Recurrent intrusive thoughts (obsessions) and repetitive behaviors or mental acts (compulsions) performed to reduce the distress those thoughts produce. OCD was reclassified from anxiety disorders to its own category in DSM-5 but shares significant mechanistic overlap.
PTSD (Post-Traumatic Stress Disorder): Also reclassified from anxiety disorders in DSM-5, PTSD involves intrusive re-experiencing of trauma, avoidance, negative alterations in cognition and mood, and hyperarousal following exposure to traumatic events.
The specific anxiety disorder you’re dealing with significantly influences which therapy will be most effective — which is why “I have anxiety” is important context but not sufficient information for optimal treatment matching.
The Hierarchy of Evidence: How to Evaluate Therapy Claims
Before diving into specific therapies, it is worth establishing how to evaluate the claims made about them — because the mental health field includes a vast range of approaches with wildly varying levels of supporting evidence.
Randomized Controlled Trials (RCTs): The gold standard of clinical evidence. Participants are randomly assigned to treatment or control conditions, and outcomes are measured systematically. Multiple RCTs showing consistent results provide strong evidence.
Meta-analyses and systematic reviews: Statistical aggregation of multiple RCTs, providing the highest level of evidence by averaging across study-specific variations.
Expert consensus and clinical guidelines: Bodies like the American Psychological Association (APA), National Institute for Health and Care Excellence (NICE), and the World Health Organization (WHO) review the evidence and issue treatment recommendations.
Clinical case series and open trials: Lower-quality evidence, but sometimes the best available for newer approaches.
Anecdotal and testimonial: No evidentiary value for treatment efficacy, though highly influential in consumer decision-making.
The therapies discussed in this article are evaluated against this hierarchy — prioritizing those with the strongest, most replicated evidence base.
The Best Therapies for Anxiety: A Research-Based Breakdown
1. Cognitive Behavioral Therapy (CBT) — The Gold Standard
If there is a single answer to “which therapy is best for anxiety,” the evidence points most consistently to Cognitive Behavioral Therapy (CBT).
CBT has accumulated the largest, most rigorous, most replicated evidence base of any psychological treatment for anxiety — across anxiety disorders in adults and children, across cultural contexts, across delivery formats (individual, group, online, self-guided), and across decades of research. It is endorsed as first-line treatment for anxiety by the APA, NICE, the WHO, and virtually every major mental health body that has reviewed the evidence.
What CBT Actually Is
CBT is not simply “talking about your thoughts.” It is a structured, time-limited, skills-based treatment that works by directly targeting the cognitive and behavioral mechanisms that maintain anxiety.
The cognitive component addresses the thought patterns that feed anxiety — the automatic worst-case interpretations, the overestimation of threat, the underestimation of coping capacity. Through a process called cognitive restructuring, clients learn to identify these patterns, evaluate the evidence for and against them, and develop more balanced, accurate interpretations.
The behavioral component — which research increasingly suggests is the more powerful of the two — directly addresses avoidance through a technique called exposure. Exposure involves approaching feared situations, sensations, or thoughts in a systematic, graded way rather than avoiding them. The mechanism is inhibitory learning — the brain learns, through direct experience, that the feared situation is safe or manageable, and this new learning gradually inhibits the old threat response.
Exposure is the single most potent element of CBT for anxiety. A meta-analysis published in the journal Psychological Bulletin found that the behavioral components of CBT — particularly exposure — account for the majority of its therapeutic effect. A CBT therapist for anxiety who is not implementing exposure is not delivering the full treatment.
What CBT Looks Like in Practice
Standard CBT for anxiety is typically delivered over 12 to 20 sessions, weekly, with each session approximately 50 minutes. Sessions follow a structured agenda: review of the previous week and homework, work on the current focus (cognitive or behavioral), assignment of between-session practice.
Between-session practice — homework — is an essential component. CBT is not a passive treatment. Change happens through deliberate practice between sessions, not just through insight during them.
The early sessions establish a shared understanding of the anxiety — its triggers, its patterns, its maintaining behaviors. The middle sessions introduce and implement the core techniques — thought challenging, behavioral experiments, exposure. The later sessions consolidate gains, prepare for setbacks, and build relapse prevention skills.
CBT for Specific Anxiety Disorders
CBT’s effectiveness varies somewhat by anxiety disorder — and specific CBT protocols have been developed for each:
GAD: CBT for GAD targets worry as a cognitive process — examining the function of worry, challenging intolerance of uncertainty, and reducing the reassurance-seeking and avoidance behaviors that maintain chronic worry. Metacognitive therapy (MCT), a CBT variant, specifically addresses beliefs about worry and is increasingly well-supported for GAD.
Panic Disorder: CBT for panic combines psychoeducation about the physiology of panic attacks (which dramatically reduces their terror once understood), interoceptive exposure (deliberately inducing the physical sensations associated with panic to build tolerance), and situational exposure to agoraphobic situations.
Social Anxiety: CBT for social anxiety targets the specific cognitive distortions of social threat, the post-event processing (rumination after social situations), and safety behaviors (the subtle ways anxious people manage social situations that paradoxically maintain anxiety). Exposure in the social context — approaching feared social situations — is central.
OCD: CBT for OCD uses a specialized form of exposure called Exposure and Response Prevention (ERP) — deliberately triggering obsessive thoughts while refraining from the compulsive responses that normally reduce them. ERP is the most effective psychological treatment for OCD by a significant margin and requires specific training to deliver effectively.
Health Anxiety: CBT for health anxiety targets reassurance-seeking behaviors (checking symptoms, researching online, seeking medical reassurance), the interpretation of normal bodily sensations as threatening, and the attentional bias toward health-related information.
2. Acceptance and Commitment Therapy (ACT) — The Powerful Alternative
ACT is the most well-established alternative to CBT for anxiety — and for many people, particularly those who have tried CBT and found it insufficiently helpful, ACT offers something qualitatively different.
ACT is part of the “third wave” of cognitive behavioral therapies — building on the behavioral and cognitive foundations of CBT but shifting the fundamental goal of treatment.
Where CBT aims to reduce anxiety by changing the content of anxious thoughts and reducing the frequency of anxiety symptoms, ACT aims to change your relationship with anxiety — learning to experience anxious thoughts and feelings without being controlled by them, while committing to behavior aligned with your values regardless of whether anxiety is present.
The Core ACT Framework
ACT is organized around six core processes, combined under two central goals: increasing psychological flexibility (the ability to be present and to move toward what matters even in the presence of difficult internal experiences) and values-based action (living in alignment with what genuinely matters to you rather than in service of anxiety reduction).
Acceptance: Rather than fighting anxiety or trying to eliminate it — which the research shows paradoxically amplifies it — ACT teaches willingness to experience anxiety as a normal human emotion that does not require immediate action or elimination.
Defusion: Changing your relationship with anxious thoughts — learning to observe them as mental events (“I’m having the thought that something terrible will happen”) rather than facts (“Something terrible will happen”). Defusion reduces the power of anxious thoughts without requiring you to change their content.
Present-moment awareness: Mindfulness of the current moment — reducing the past-focused and future-focused nature of anxiety by grounding attention in what is actually happening right now.
Self as context: Developing a stable sense of self that is larger than any thought, feeling, or experience — a perspective from which anxiety can be observed without being identified with.
Values clarification: Identifying what genuinely matters to you — what kind of person you want to be, what kind of relationships you want, what you want to contribute — as a compass for action.
Committed action: Taking specific, concrete steps in the direction of your values, even in the presence of anxiety. Expanding your life rather than contracting it around anxiety.
When ACT Is Particularly Well-Suited
ACT is especially valuable when:
Anxiety is entangled with existential questions — about meaning, identity, or values — that CBT’s more technique-focused approach doesn’t fully address.
Previous CBT has been tried but the person remains stuck in a struggle with anxiety rather than moving forward despite it.
The person has a strong mindfulness capacity or is drawn to a more philosophical approach to their difficulties.
Anxiety is significantly affecting their engagement with valued life activities — because ACT’s values-based framework directly targets this dimension.
The evidence base for ACT in anxiety is strong and growing — multiple meta-analyses have found ACT to be comparable to CBT in effectiveness for anxiety disorders, with some evidence of particular advantages for GAD and mixed anxiety presentations.
3. Exposure and Response Prevention (ERP) — The Essential Treatment for OCD
If your anxiety manifests primarily as OCD — intrusive thoughts paired with compulsive rituals performed to reduce the distress those thoughts generate — the specific treatment you need is Exposure and Response Prevention (ERP).
ERP is not simply CBT for OCD. It is a specialized protocol that requires specific training and that works through a mechanism distinct from standard cognitive techniques.
The core of ERP is straightforward in description and profoundly challenging in practice: deliberately expose yourself to the triggers that produce obsessive thoughts (the exposure component) while refraining from the compulsive responses that normally reduce the associated distress (the response prevention component).
The mechanism is inhibitory learning — your brain learns, through repeated experience, that the obsessive thought does not produce the feared outcome and that the distress it generates is survivable without compulsive action. Over time, this new learning inhibits the old obsession-compulsion cycle.
ERP requires a therapist who is specifically trained in its delivery — the pacing of exposure hierarchy, the management of accommodation behaviors, the handling of mental compulsions (which are invisible and therefore easy to miss), and the maintenance of appropriate challenge without overwhelming distress.
Research on ERP for OCD is among the most robust in psychotherapy — with response rates in specialized ERP programs reaching 60-85%. If you have OCD and have not received proper ERP treatment, you may not yet have received the treatment most likely to help you.
4. EMDR — For Anxiety With Trauma Roots
Eye Movement Desensitization and Reprocessing (EMDR) was originally developed for PTSD and is the most extensively evidence-supported treatment for trauma-related anxiety. But its relevance extends beyond PTSD to any anxiety disorder with identifiable traumatic or adverse experience roots.
EMDR works through a process of bilateral stimulation (typically eye movements, but sometimes taps or tones) while the client holds in mind specific aspects of a traumatic memory — the image, the associated negative belief, the body sensation. The bilateral stimulation appears to facilitate the processing of traumatic memories in a way that reduces their emotional intensity and integrates them into the broader autobiographical narrative.
The precise neurological mechanism of EMDR remains somewhat debated — whether the bilateral stimulation itself is the active ingredient or whether the structured processing protocol is the key. What is not debated is the evidence for its effectiveness — multiple meta-analyses have confirmed EMDR’s efficacy for PTSD and trauma-related anxiety, and it is endorsed as a first-line trauma treatment by the WHO and APA.
When EMDR Is the Right Choice for Anxiety
EMDR is particularly indicated when:
Your anxiety has identifiable origins in specific traumatic events or adverse childhood experiences.
Trauma memories or flashbacks are a significant feature of your anxiety presentation.
You have tried CBT without achieving the expected improvement and trauma may be a maintaining factor.
Your anxiety includes significant somatic components — body-based sensations and reactions — that feel disconnected from conscious cognitive processing.
Standard CBT can be limited in its effectiveness for anxiety that is deeply rooted in trauma. EMDR addresses the trauma at its source in a way that cognitive techniques do not, and the anxiety reduction follows from the trauma processing.
5. Dialectical Behavior Therapy (DBT) — For Anxiety With Emotional Dysregulation
DBT was originally developed for Borderline Personality Disorder but has been adapted and researched for anxiety disorders — particularly those characterized by intense emotional dysregulation, self-destructive coping behaviors, and interpersonal instability.
If your anxiety is accompanied by intense, rapidly shifting emotions that are difficult to manage — if your anxiety frequently escalates to crisis level, if you have used self-harm, substance use, or other destructive behaviors to manage anxious states — DBT’s comprehensive skill set may be more appropriate than standard CBT.
DBT’s four skill modules — mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness — provide a comprehensive toolkit for managing the emotional intensity that underlies anxiety in this presentation. The distress tolerance skills in particular (TIPP, radical acceptance, half-smiling) offer immediate, in-the-moment tools for managing acute anxiety states without making the situation worse.
6. Mindfulness-Based Cognitive Therapy (MBCT) — For Recurrent and Chronic Anxiety
MBCT combines mindfulness meditation practice with cognitive therapy techniques in an eight-week group program originally developed for recurrent depression but now well-researched for anxiety.
MBCT’s core mechanism is decentering — learning to observe thoughts and feelings as passing mental events rather than facts requiring action. This is similar to ACT’s defusion concept and addresses the same fundamental problem: the tendency to fuse with anxious thoughts and to respond to them as if they represent objective reality.
MBCT is particularly valuable as a maintenance intervention — something to continue practicing after acute treatment has produced initial improvement, to sustain gains and prevent relapse. Research consistently shows that MBCT reduces relapse rates for both depression and anxiety more effectively than treatment as usual.
7. Psychodynamic Therapy — For Anxiety With Deep Developmental Roots
Psychodynamic therapy has a smaller but growing evidence base for anxiety — and for specific presentations, it offers something that CBT and ACT do not fully provide.
Psychodynamic approaches work with the deeper, often unconscious patterns — rooted in early relationships and developmental experiences — that shape current emotional experience and relational patterns. For anxiety that is deeply entangled with attachment wounds, early relational trauma, identity questions, and patterns that repeat across relationships and contexts, psychodynamic work addresses the roots rather than the branches.
Accelerated Experiential Dynamic Psychotherapy (AEDP) and Short-Term Psychodynamic Psychotherapy (STPP) are among the more evidence-supported variants for anxiety. Research meta-analyses have found psychodynamic therapy produces outcomes comparable to CBT for anxiety — with effects that continue to improve after treatment ends, possibly because psychodynamic work produces structural personality change rather than just symptom reduction.
Psychodynamic therapy is typically longer-term than CBT and less structured — which may be a disadvantage for people who need relatively quick symptomatic relief, but an advantage for those whose anxiety is embedded in complex developmental history that structured technique-based approaches don’t reach.
8. Internal Family Systems (IFS) — The Emerging Approach for Complex Anxiety
IFS, developed by Dr. Richard Schwartz, is gaining significant clinical traction for anxiety — though its formal evidence base is less developed than CBT’s.
IFS works with different “parts” of the internal system — the anxious part, the inner critic, the protector, the people-pleaser — as a way of understanding and healing the internal conflicts that produce and maintain anxiety. The core premise is that what we call anxiety is often a “protective part” of the system doing its best to keep a more vulnerable part safe — and that working compassionately with that protective part, rather than trying to eliminate it, produces more lasting change.
IFS is particularly valuable for anxiety that:
Feels ego-syntonic — that is, feels like part of who you are rather than a foreign intrusion.
Is entangled with perfectionism, people-pleasing, and chronic self-criticism.
Has not responded to more behavioral approaches because the deeper emotional roots remain unaddressed.
Involves significant shame — IFS’s Self-compassion-based approach is particularly well-suited to working with shame without amplifying it.
How to Choose the Right Therapy for Your Specific Anxiety: A Decision Framework
With all of these options available, how do you actually decide what to pursue? Here is a practical framework:
If you have a specific, identifiable anxiety disorder (panic disorder, social anxiety, specific phobia, health anxiety, GAD) and have not previously tried evidence-based treatment: Start with CBT. It has the broadest evidence base, the clearest treatment protocols, and the most therapists trained in its delivery.
If you have OCD: Seek ERP specifically — not generic CBT, not DBT, not ACT as a standalone. ERP is the treatment, and you need a therapist specifically trained in it.
If your anxiety has clear trauma roots or PTSD features: Prioritize EMDR alongside or before standard CBT. Treating the trauma reduces the anxiety more efficiently than treating the anxiety while the trauma remains unprocessed.
If you’ve tried CBT and it helped but didn’t fully resolve things — or if you’re stuck fighting your anxiety rather than living alongside it: Consider ACT. Its acceptance-based framework often reaches something CBT’s change-focused approach doesn’t.
If your anxiety is accompanied by intense emotional dysregulation, self-destructive coping, or significant interpersonal turbulence: DBT may be more appropriate than standard CBT.
If your anxiety feels deeply entangled with who you are, your early history, or complex relational patterns: Psychodynamic therapy or IFS may address the roots more effectively than technique-focused approaches.
If you want to sustain gains made in acute treatment and prevent relapse: Add MBCT as an ongoing practice.
If you’re not sure: Start with a comprehensive assessment from a skilled clinician who can help you identify the right starting point based on your specific presentation.
Does Online Therapy Work as Well as In-Person for Anxiety?
This is one of the most frequently asked questions about online anxiety treatment — and the research answer is now quite clear.
Multiple systematic reviews and meta-analyses have found that online CBT for anxiety produces outcomes comparable to in-person CBT — across anxiety disorders, across age groups, and across delivery formats (therapist-delivered video, therapist-delivered phone, and even guided self-help digital programs).
The therapeutic alliance — which as established earlier is the primary predictor of therapy outcomes — transfers effectively to online formats. The skills learned in online CBT are as effectively acquired as those learned in person. The exposure work that is the core of behavioral anxiety treatment can be conducted in the real-world environments where anxiety is triggered — which online therapy, paradoxically, may facilitate more naturally than in-office treatment.
For anxiety specifically, online therapy offers additional advantages. Social anxiety treatment benefits from the reduced initial exposure of video versus in-person interaction. Agoraphobia treatment allows the person to begin from a safe environment and gradually approach feared situations in the real world. Health anxiety treatment removes the clinic environment that might itself be a trigger.
The evidence is unambiguous: if the choice is between online therapy with the right therapist and in-person therapy with the wrong one, choose the right therapist online every time.
What About Medication? How It Fits With Therapy for Anxiety
This guide is focused on therapy — but it would be incomplete without addressing the relationship between therapy and medication, because the question “should I do therapy or medication?” is one of the most common questions people with anxiety ask.
The honest answer is: for moderate to severe anxiety, therapy plus medication often produces better outcomes than either alone.
SSRIs (Selective Serotonin Reuptake Inhibitors) — including sertraline (Zoloft), escitalopram (Lexapro), and fluoxetine (Prozac) — are the first-line pharmacological treatment for most anxiety disorders. They reduce the baseline level of anxious arousal, which makes the cognitive and behavioral work of therapy more accessible.
SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors) — including venlafaxine (Effexor) and duloxetine (Cymbalta) — are similarly effective and are the first-line recommendation for GAD specifically.
Benzodiazepines (Xanax, Valium, Klonopin) are fast-acting but are not recommended for long-term anxiety treatment due to dependence risk, tolerance development, and evidence that they may actually interfere with the inhibitory learning that makes exposure therapy effective.
The most important thing to understand about medication for anxiety is that it is most effective when used alongside therapy — not instead of it. Medication reduces symptoms; therapy changes the underlying patterns that produce them. Both matter.
Get Matched With the Right Anxiety Therapist Through IGOTU Corp
Understanding which therapy is best for your anxiety is an important first step. Actually accessing that therapy — finding a qualified therapist, navigating insurance, managing wait lists, evaluating fit, and beginning treatment — is where most people get stuck.
IGOTU Corp removes those barriers.
IGOTU Corp connects people with anxiety with licensed, vetted mental health professionals trained in the specific evidence-based approaches that produce real outcomes — CBT, ERP, EMDR, ACT, DBT, and more. Their clinician network is specifically screened for anxiety specialization, not just general mental health experience.
Their matching process goes beyond availability. It considers your specific anxiety presentation, your treatment history, your preferences about approach, and your practical needs — to connect you with the therapist most likely to be genuinely helpful for your specific situation.
Whether you are dealing with generalized anxiety that has been with you for years, panic attacks that have started recently, social anxiety that has been quietly limiting your life, OCD that has never been properly treated, or PTSD-rooted anxiety that previous therapy hasn’t reached — IGOTU Corp’s licensed therapist network is equipped to meet you exactly where you are.
Visit IGOTU Corp today, take their free anxiety assessment, and get matched with a licensed therapist who specializes in the specific type of anxiety you’re dealing with. Because the research is clear on what works — and you deserve access to it, without spending months navigating a system that wasn’t designed to make itself easy.
How Long Does Therapy for Anxiety Take to Work?
This is one of the most practically important questions people ask — and the research provides reasonably clear answers.
CBT for specific anxiety disorders — panic disorder, specific phobias, social anxiety — typically produces meaningful symptom reduction within 12 to 20 sessions, with some presentations responding in as few as 8 sessions. Panic disorder in particular tends to respond relatively quickly to CBT with interoceptive exposure.
GAD tends to require somewhat longer treatment — 16 to 24 sessions typically — because it is by definition a pervasive, multi-domain condition rather than a circumscribed fear response.
OCD with ERP shows meaningful response within 12 to 20 sessions of intensive ERP, with more severe presentations requiring longer treatment and sometimes residential or intensive outpatient programs.
PTSD with EMDR — the research suggests meaningful improvement within 8 to 12 EMDR sessions for single-incident trauma, with complex or developmental trauma requiring longer treatment.
ACT typically runs 8 to 16 sessions for anxiety, though some people continue longer for deeper values and identity work.
Early response — some perceptible shift in symptoms within the first 4 to 8 sessions — is a positive prognostic indicator. Research consistently shows that early symptom movement predicts better final outcomes. If you are at session 8 or 10 with no perceptible change, that is worth raising directly with your therapist.
What these timelines have in common is that they are months, not years — with the exception of longer-term psychodynamic work for deeply rooted presentations. Anxiety is among the most treatment-responsive conditions in psychiatry. The right treatment, delivered competently, produces real change in a clinically meaningful timeframe.
What If Therapy Hasn’t Worked for You Before?
This is a critically important question because a significant number of people seeking anxiety treatment have already tried therapy — and found it didn’t help, or didn’t help enough.
Before concluding that therapy doesn’t work for your anxiety, it is worth evaluating what kind of therapy you received:
Was it evidence-based for your specific anxiety disorder? General supportive counseling is not the same as CBT. Talk therapy without structured behavioral techniques is not the same as ERP. Many people who have “tried therapy for anxiety” have not received the specific, structured, evidence-based protocols that the research supports.
Did it include exposure work? If your therapy for anxiety never involved approaching feared situations, sensations, or thoughts in a systematic way — it did not include the most potent element of anxiety treatment. Cognitive work without behavioral exposure produces more limited outcomes.
Was the therapeutic relationship right? A poor therapeutic fit produces poor outcomes regardless of the modality. A previous unhelpful therapy experience is evidence that particular therapist or approach wasn’t right for you — not that therapy doesn’t work for anxiety.
Was it long enough? Anxiety that has been present for years does not resolve in four sessions. An inadequate trial of an appropriate treatment is different from an adequate trial that didn’t work.
Did it address the right level of the problem? If your anxiety has deep trauma roots, CBT without trauma processing may reduce surface symptoms without touching the driving mechanism. If it has strong somatic components, purely cognitive approaches may be insufficient.
Most people who have had unhelpful previous therapy for anxiety have not yet had the right therapy for their specific presentation. The right treatment, from the right therapist, looks qualitatively different.
Therapy for Anxiety in Specific Populations: Important Considerations
Anxiety Therapy for Adolescents and Young Adults
CBT is well-established as effective for anxiety in adolescents — with specific adaptations for developmental stage, including more parental involvement for younger adolescents and attention to the identity and social developmental tasks of late adolescence and young adulthood. Early intervention for adolescent anxiety produces significantly better long-term outcomes than waiting until adulthood.
Anxiety Therapy for Older Adults
Anxiety is among the most prevalent mental health conditions in older adults — and among the most undertreated, partly because older adults present with more somatic anxiety symptoms that are attributed to physical health conditions, and partly because they are less likely to seek mental health treatment. CBT adapted for older adults — with slower pacing, attention to cohort-specific beliefs about mental health treatment, and integration of life review — is effective and warranted.
Anxiety Therapy for People of Color in California
California’s racial and ethnic diversity makes culturally responsive therapy not an optional add-on but a clinical necessity. Research consistently shows that therapy outcomes are better when there is cultural concordance between therapist and client — and when the therapist has specific training in culturally responsive care. Seek therapists who explicitly address cultural factors, who have experience with your specific community, and who do not require you to explain your cultural context from scratch in every session.
Anxiety Therapy During Pregnancy and Postpartum
Anxiety is extremely common during pregnancy and the postpartum period — and is significantly underdiagnosed and undertreated in these populations. CBT and ACT adapted for perinatal anxiety are effective and should be considered before medication during pregnancy and breastfeeding, though medication decisions should be made in consultation with a psychiatrist and OB. Postpartum anxiety specifically requires a therapist with perinatal mental health training.
Frequently Asked Questions (FAQs) About the Best Therapy for Anxiety
Q: Is CBT or medication better for anxiety? The research does not clearly favor one over the other for most anxiety disorders. Both are effective. Combined treatment — CBT plus medication — produces better outcomes than either alone for moderate to severe presentations. CBT produces more durable changes that persist after treatment ends; medication effects typically require ongoing use to be maintained. For mild to moderate anxiety, CBT alone is often sufficient and preferable due to its durability and absence of side effects.
Q: How many therapy sessions do I need for anxiety? Most people with anxiety disorders require 12 to 20 sessions of CBT to achieve meaningful, durable improvement. Simpler, more circumscribed presentations (specific phobias) may respond in fewer sessions. More complex presentations (GAD, OCD, PTSD-rooted anxiety) typically require more. The research suggests that treatment should continue until symptom reduction is substantial and maintained — not stopped at a pre-set number of sessions.
Q: Can anxiety be cured with therapy? “Cured” is not the most accurate framing. A more accurate description is that effective therapy produces remission — a state in which anxiety is no longer clinically significant, no longer impairing functioning, and no longer driving avoidance and suffering. Many people who complete evidence-based anxiety treatment remain in remission indefinitely. Some experience recurrence during major stressors — but with the tools from therapy, are better equipped to manage and recover from those recurrences.
Q: Is online therapy effective for anxiety? Yes — unambiguously and substantially. Multiple systematic reviews confirm that online CBT for anxiety produces outcomes comparable to in-person CBT, across anxiety disorders and delivery formats. The therapeutic alliance, the skills acquisition, and the behavioral change that produce anxiety improvement all transfer effectively to online formats.
Q: What is the fastest therapy for anxiety? For circumscribed anxiety disorders, intensive CBT formats — multiple sessions per week or intensive one-week programs — produce faster results than standard weekly therapy. Single-session interventions have been researched for specific phobias and show meaningful effects. For most anxiety disorders, significant improvement within 8 to 12 weekly sessions is achievable with high-quality CBT. Panic disorder in particular often responds rapidly to CBT with interoceptive exposure.
Q: Can therapy make anxiety worse before it gets better? Temporarily, yes — particularly in the early stages of exposure-based treatment. Approaching feared situations deliberately produces short-term increases in anxiety before the inhibitory learning that reduces anxiety has had time to occur. This is expected, normal, and a sign that the treatment is engaging the right mechanism. A good therapist will prepare you for this and calibrate the pace to keep the discomfort within the range that facilitates learning without overwhelming you.
Q: What type of therapist is best for anxiety? Any licensed mental health professional — LCSW, LMFT, LPCC, psychologist — can be an effective anxiety therapist if they have specific training in evidence-based anxiety treatment. The license type matters less than the specific training in CBT, ERP, EMDR, or ACT for anxiety. Verify both licensure and specific anxiety training before committing to a therapist.
Q: Does CBT work for all types of anxiety? CBT is effective across all anxiety disorders, but specific CBT protocols are more appropriate for specific presentations. CBT for GAD, CBT for panic, CBT for social anxiety, and ERP for OCD are distinct protocols — not interchangeable. A skilled CBT therapist for anxiety will know which protocol applies to your presentation and will deliver that specific protocol rather than generic CBT.
Q: What should I do if I can’t afford therapy for anxiety? Options for lower-cost anxiety therapy include sliding-scale fees (ask therapists directly), pre-licensed therapists under supervision, university training clinics, community mental health centers, and structured digital CBT programs. IGOTU Corp can help identify therapists whose fees align with your financial situation. Self-help workbooks based on CBT provide meaningful support for those who cannot access formal therapy.
Q: How do I get started with evidence-based anxiety therapy through IGOTU Corp? Visit IGOTU Corp, complete their free anxiety assessment, and their clinical matching process will connect you with a licensed therapist trained in the specific evidence-based approach most appropriate for your anxiety presentation. IGOTU Corp takes the overwhelming part out of finding the right help — so you can spend your energy on getting better, not on navigating a system that wasn’t designed to be easy. Visit IGOTU Corp today to get started.
The Bottom Line: Anxiety Is Highly Treatable — With the Right Therapy
Anxiety is not a character flaw. It is not evidence of weakness. It is not something you should simply push through, manage better, or accept as a permanent feature of your life.
It is a neurobiological condition — well understood, extensively researched, and highly responsive to the right treatment. The research on anxiety therapy is among the most consistent in all of psychiatry: the right therapy, delivered competently, produces real, meaningful, lasting change in the majority of people who receive it.
What the research is clear on: CBT is the gold standard, with the broadest evidence base across anxiety disorders. ERP is essential for OCD. EMDR addresses trauma-rooted anxiety in ways that cognitive approaches alone cannot. ACT offers something different and valuable for people stuck in the struggle with anxiety rather than moving forward despite it. The relationship with your therapist matters as much as the modality. And early, appropriate treatment produces better long-term outcomes than years of suffering followed by eventual help.
What this means for you: if you are living with anxiety — whether it has been weeks or decades — the treatment that gives you your life back is not theoretical. It exists. It is accessible. And you deserve access to it delivered by a clinician who genuinely knows what they’re doing.
IGOTU Corp’s licensed, anxiety-specialist therapists are ready to provide exactly that. Visit IGOTU Corp today — take the free anxiety assessment, get matched with the right therapist for your specific presentation, and begin the treatment that the research shows most people with anxiety are genuinely capable of recovering through.
Because anxiety has already taken enough from you. It is time to take it back.
Recent Posts
Related Posts
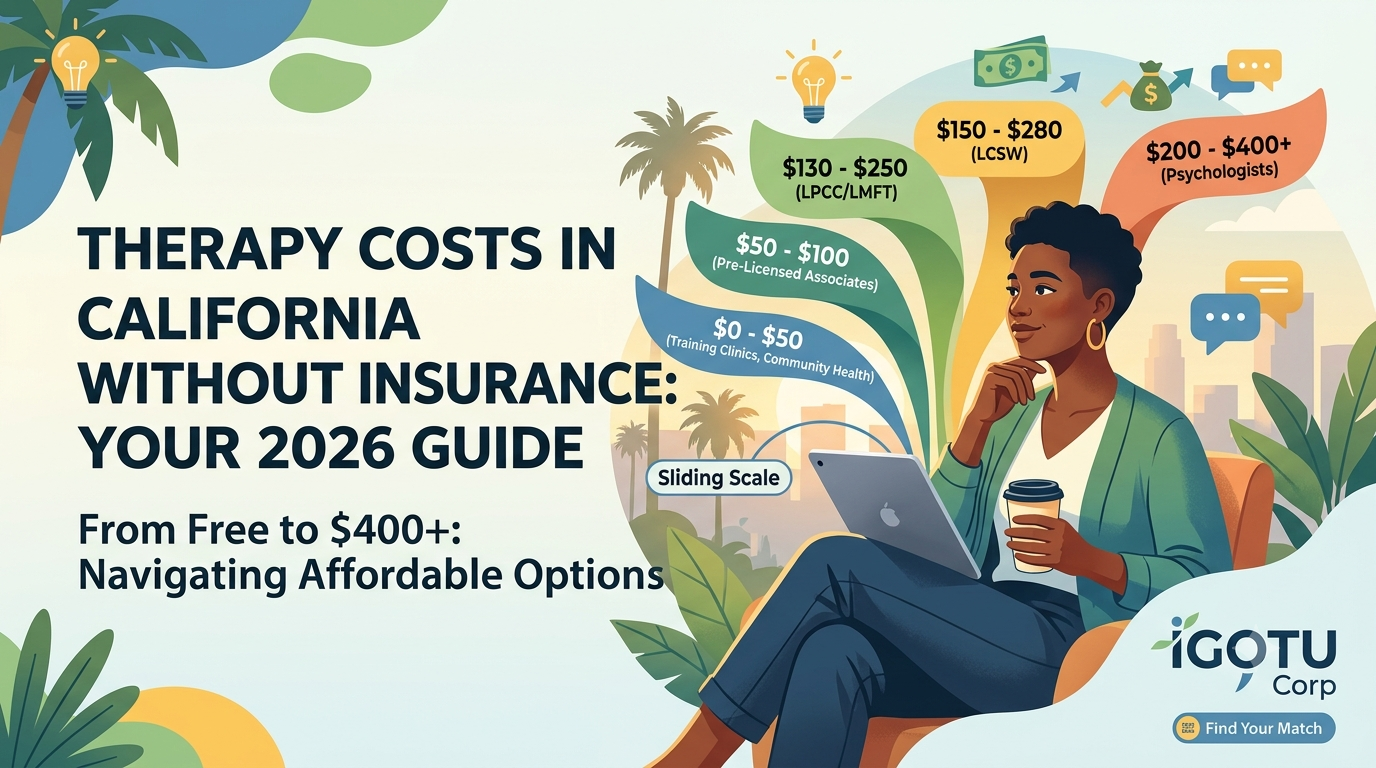
What is the Cost of Therapy Without Insurance in California?
Here is the direct answer: therapy without insurance in California in 2026 costs between $0 and $400 per session, depending...
California ESA Laws Explained: 30-Day Rule for Valid
California ESA Laws Changed. Most People Don't Know It Yet. If you have been researching Emotional Support Animals in...

Why Do I Feel Lonely and Depressed? Understanding the Connection
Quick answer: Why do I feel lonely and depressed? Learn the real neurological connection between loneliness and depression, what...

Why I Feel Stressed All the Time? Causes and Treatment
QUICK ANSWER: Feeling stressed all the time is not just a personality trait or a busy life — it is...
Understanding Functional Depression: The Silent Struggle
The Depression Nobody Notices — Including Sometimes You You got up this morning. You made coffee. You answered your...